
We’ve Been Blaming Cholesterol for Heart Disease for 60 Years. What If We’re Wrong?
For decades, we’ve been told a simple story:
Saturated fat raises cholesterol.
Cholesterol clogs arteries.
Clogged arteries lead to heart attacks.
It’s clear. It’s logical. It’s widely accepted. But there’s just one problem: The full body of evidence doesn’t support the simplicity of that story.
And if we’ve been targeting the wrong culprit… We may be missing what actually drives heart disease.
The Origins of the Lipid Hypothesis
The lipid–heart hypothesis offered something powerful: simplicity. It gave us a measurable target. A clear villain. A straightforward intervention.
Lower cholesterol → reduce risk → prevent disease.
But human biology rarely operates in straight lines. Over the same decades that low-fat messaging dominated, we saw a dramatic rise in:
- Obesity
- Type 2 diabetes
- Insulin resistance
- Metabolic dysfunction
Which raises a critical question: Did we mistake a marker for a cause?

What the Research Actually Shows
Large-scale data has consistently challenged the simplicity of the saturated fat narrative. A meta-analysis of nearly 347,000 individuals found no significant association between saturated fat intake and cardiovascular disease (Siri-Tarino et al., 2010). The Women’s Health Initiative—one of the largest dietary trials ever conducted—showed that reducing fat intake did not significantly reduce heart disease or stroke risk (Howard et al., 2006). The Nurses’ Health Study similarly demonstrated that simply lowering total fat intake did not produce the expected reductions in cardiovascular outcomes (Hu et al., 2001).
This doesn’t mean diet doesn’t matter. It means: The story is more complex than “fat is bad.”
Cholesterol: Essential, Not Optional
Cholesterol is not a toxin. It is a biological necessity. Every single cell in your body depends on it for structure and function. Without cholesterol, cellular integrity breaks down.
Cholesterol plays a critical role in:
- Cell membrane stability
- Hormone production
- Brain structure and function
- Vitamin D synthesis
- Fat digestion
Your body produces the majority of its cholesterol because it needs it to survive. So the real question becomes: If cholesterol is essential… why are we treating it as the primary enemy?
How High Is “High Cholesterol”?
Not long ago, total cholesterol above 280 mg/dL was considered high.
Then it became:
- 250 mg/dL
- 220 mg/dL
- 200 mg/dL
- And now, in some cases, even 130–160 mg/dL is considered optimal
Each time the threshold is lowered, millions more people become candidates for medication. This doesn’t automatically invalidate the guidelines—but it does raise an important question: Are we redefining risk—or redefining normal?

From Framingham to HUNT 2: A Critical Shift
Much of modern cholesterol theory traces back to early findings from the Framingham Heart Study, which identified an association between cholesterol levels and heart disease risk.
But association is not causation. And as longer-term data accumulated—and broader populations were studied—the narrative began to evolve.
The HUNT 2 study, one of the largest population-based health studies, revealed:
- The relationship between cholesterol and mortality is not linear
- In many populations—particularly women—higher cholesterol was not associated with increased mortality
- In some cases, lower cholesterol was associated with higher mortality
Even more telling:
- The predictive value of cholesterol declines with age
- In older adults, higher cholesterol is often associated with equal or better survival outcomes
When you step back and look at the full body of evidence—from Framingham to HUNT 2 and beyond—the conclusion becomes difficult to ignore: Cholesterol alone does not adequately explain cardiovascular disease.
A Critical Reframe: Cholesterol as a Response
If cholesterol isn’t the primary driver, what is it?
Emerging evidence suggests a different model: Cholesterol may be part of the body’s response to damage—not the root cause of it.
For example:
- Inflammation damages blood vessels
- The body sends lipoproteins (like LDL) to help repair that damage
- Over time, this repair process can contribute to plaque formation
In this context, cholesterol behaves less like a villain—And more like a repair molecule responding to injury. This aligns with decades of research showing that inflammation—not cholesterol alone—is central to atherosclerosis.

Why Cholesterol Levels Rise
Elevated cholesterol is often blamed on diet alone. But the reality is far more complex.
Key drivers include:
Inflammation – The underlying trigger of vascular damage.
Blood Sugar Dysregulation – High glucose and insulin levels damage arteries and alter lipid behavior.
Liver Function – The liver regulates cholesterol production and clearance.
Metabolic Dysfunction – Insulin resistance is a major contributor to cardiovascular risk.
Lifestyle Factors – Sleep, stress, hydration, and movement all influence metabolic health.
Cholesterol and Longevity: A More Nuanced Reality
Some of the most overlooked data in this conversation comes from longevity research.
Findings across multiple studies suggest:
- Many heart attack patients have normal cholesterol levels
- In older populations, higher cholesterol is often associated with longer lifespan
- Very low cholesterol levels have been linked to increased mortality in certain groups
This doesn’t mean higher is always better. But it does mean: The relationship between cholesterol and health is not simple—and not universal.
The Limits of a Single Biomarker
LDL cholesterol is useful. But it is only one piece of a much larger puzzle.
True cardiovascular risk is influenced by:
- Inflammation
- Insulin resistance
- Triglycerides
- HDL levels
- Lifestyle factors
Because ultimately: Health is determined by systems—not single numbers.

Rethinking the “War” on Cholesterol
For decades, the dominant strategy has been straightforward: Lower cholesterol—often with medication. Statins are now among the most widely prescribed drugs in the world. As thresholds have lowered, eligibility has expanded—bringing millions more into treatment.
At face value, this approach makes sense:
Lower cholesterol → reduce risk → improve outcomes.
But the data tells a more nuanced story.
Do Lower Numbers Always Translate to Better Outcomes?
Statins are highly effective at lowering LDL cholesterol. That’s not in question. The more important question is: Do they consistently improve meaningful long-term outcomes—especially in lower-risk individuals?
Independent analyses have found:
- Benefits in primary prevention are often modest
- Absolute risk reduction is small
- Improvements in overall mortality are inconsistent
In other words: Lowering a number does not automatically translate into better health outcomes.
Treating Risk Factors vs. Root Causes
As cholesterol thresholds have dropped, more individuals have been classified as candidates for medication.
But this raises a critical question: Are we treating risk factors—or are we addressing root causes?
Because lowering a biomarker does not resolve:
- Inflammation
- Insulin resistance
- Insulin resistance
- Metabolic dysfunction
Understanding the Trade-Offs
Statins are not without consequences. While many tolerate them well, documented side effects include:
- Muscle damage (myotoxicity)
- Nerve-related symptoms
- Liver dysfunction
- Endocrine disruption
- Cardiotoxicity
- Increased risk of diabetes
These effects are not universal. But they are real. And they matter when evaluating risk vs. benefit at scale.
A More Balanced Perspective
This is not about rejecting conventional medicine. It’s about contextualizing it. Statins can be valuable tools—especially in higher-risk individuals. But they are not a universal solution.
And they do not replace the importance of addressing the deeper drivers of health:
- Inflammation
- Blood sugar regulation
- Metabolic function
- Lifestyle patterns
Because ultimately: You cannot medicate your way out of a lifestyle-driven condition.
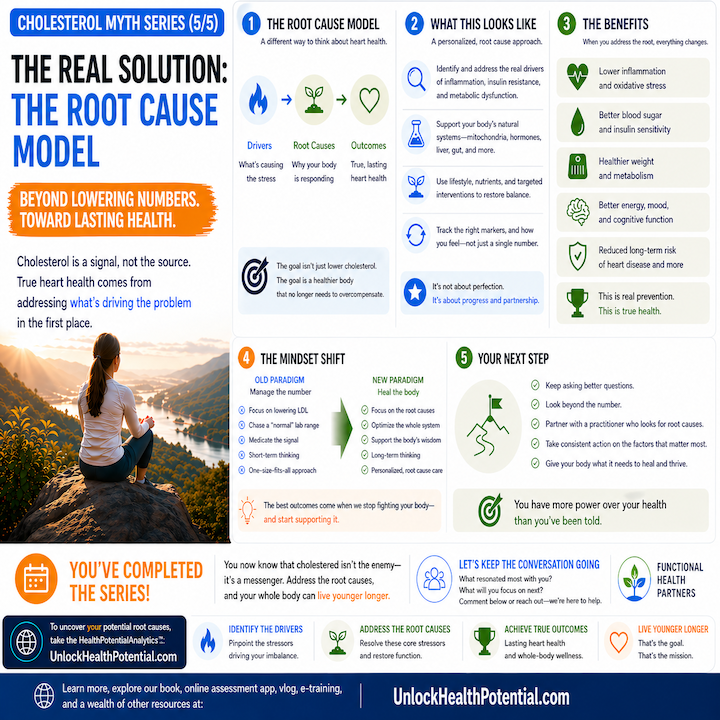
Moving Beyond a Single-Target Approach
When cholesterol becomes the primary focus, we risk missing the bigger picture. True cardiovascular health is not defined by one number—It is shaped by a network of interconnected systems.
And when we shift from a narrow, number-driven model to a root-cause, systems-based approach, we unlock a far more powerful path forward.
The Bottom Line
We’ve spent decades chasing a number. But real health was never about a single biomarker. It’s about understanding the system your body operates in—and addressing the root causes that actually drive disease.
If this shifted your perspective, don’t keep it to yourself. Share it with someone who’s been told to fear their cholesterol.
And if you’re ready to go deeper—to understand your body beyond surface-level labs—that’s exactly what we focus on at UnlockHealthPotential.com. Because the goal isn’t just to live longer. It’s to live younger, longer.
FAQs
Cholesterol is associated with cardiovascular risk, but current research suggests the relationship is more complex than simply “high cholesterol causes heart disease.” Factors such as inflammation, insulin resistance, metabolic dysfunction, blood sugar regulation, and lifestyle patterns also play major roles in cardiovascular health.
Not necessarily. Studies have found that the relationship between cholesterol and health is not always linear. In some populations—particularly older adults and women—higher cholesterol levels have not consistently been associated with increased mortality. Cholesterol levels should always be interpreted within the context of overall health and risk factors.
Cholesterol is essential for life. It helps build cell membranes, produce hormones, synthesize vitamin D, support brain function, and aid in fat digestion. In fact, the body manufactures most of its own cholesterol because it is required for normal biological function.
Research increasingly points to inflammation, insulin resistance, metabolic dysfunction, elevated blood sugar, smoking, poor sleep, chronic stress, lack of physical activity, and other lifestyle factors as important contributors to cardiovascular disease. Cholesterol is only one piece of a much larger picture.
Yes. Supporting cardiovascular health often involves addressing root causes such as chronic inflammation, blood sugar instability, excess body fat, poor sleep, stress, physical inactivity, and nutrient deficiencies. A systems-based approach can help improve overall metabolic and cardiovascular health rather than focusing on a single biomarker.
This content is for educational purposes only and is not intended as medical advice.
Scientific References
Björnsson E. Hepatotoxicity associated with statins. Liver International. 2017 37(2):173–178.
https://pubmed.ncbi.nlm.nih.gov/27716967/
Chaulin A. Cardiotoxicity as a Possible Side Effect of Statins. Rev Cardiovasc Med. 2023 Jan 11 24(1):22. doi: 10.31083/j.rcm2401022. PMID: 39076865 PMCID: PMC11270446. https://pmc.ncbi.nlm.nih.gov/articles/PMC11270446/
Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. New England Journal of Medicine.2005 352(16):1685–1695. https://pubmed.ncbi.nlm.nih.gov/15745999/
Howard BV, Van Horn L, Hsia J, et al. Low-fat dietary pattern and risk of cardiovascular disease: the Women’s Health Initiative randomized controlled dietary modification trial. Journal of the American Medical Association.2006 295(6):655–666. https://pubmed.ncbi.nlm.nih.gov/16467234/
Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk of coronary heart disease in women. New England Journal of Medicine. 2001 345(11):790–797. https://pubmed.ncbi.nlm.nih.gov/11301006/
Jacobs D, Blackburn H, Higgins M, et al. Report of the conference on low blood cholesterol: mortality associations. Circulation. 1992 86(3):1046–1060. https://pubmed.ncbi.nlm.nih.gov/1737601/
Kannel WB, Castelli WP, Gordon T, McNamara PM. Serum cholesterol, lipoproteins, and the risk of coronary heart disease: the Framingham Study. Annals of Internal Medicine. 1971 74(1):1–12. https://pubmed.ncbi.nlm.nih.gov/5107701/
Libby P. Inflammation in atherosclerosis. Circulation. 2002 105(9):1135–1143. https://pubmed.ncbi.nlm.nih.gov/12119242/
Marcoff L, Thompson PD. The role of coenzyme Q10 in statin-associated myopathy. Journal of the American College of Cardiology. 2007 49(23):2231–2237. https://pubmed.ncbi.nlm.nih.gov/17643597/
MedCrave Online Journal of Cardiology and Current Research. From Framingham to HUNT 2: 60 years blaming the wrong culprit? https://medcraveonline.com/JCCR/from-framingham-to-hunt-2-60-years-blaming-the-wrong-culprit.html
Ravnskov U, Diamond DM, Hama R, et al. Lack of an association or an inverse association between low-density lipoprotein cholesterol and mortality in the elderly: a systematic review. BMJ Open. 2016 6:e010401. https://pubmed.ncbi.nlm.nih.gov/27292972/
Rojas-Fernandez CH, Cameron JC. Is statin-associated cognitive impairment clinically relevant? Annals of Pharmacotherapy. 2012 46(4):549–557. https://pubmed.ncbi.nlm.nih.gov/22274654/
Sachdeva A, Cannon CP, Deedwania PC, et al. Lipid levels in patients hospitalized with coronary artery disease: an analysis of 136,905 hospitalizations. American Heart Journal. 2009 157(1):111–117.
https://pubmed.ncbi.nlm.nih.gov/19081406/
Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomized statin trials. The Lancet. 2010 375(9716):735–742. https://pubmed.ncbi.nlm.nih.gov/20167359/
Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. American Journal of Clinical Nutrition. 2010 91(3):535–546. https://pubmed.ncbi.nlm.nih.gov/20071648/
Taylor F, Huffman MD, Macedo AF, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews. 2013. https://pubmed.ncbi.nlm.nih.gov/23440795/
Thompson PD, Panza G, Zaleski A, Taylor B. Statin-associated side effects. Journal of the American College of Cardiology. 2016 67(20):2395–2410. https://pubmed.ncbi.nlm.nih.gov/27712900/
Turner RM, Pirmohamed M. Statin-Related Myotoxicity: A Comprehensive Review of Pharmacokinetic, Pharmacogenomic and Muscle Components. J Clin Med. 2019 Dec 20 9(1):22. doi: 10.3390/jcm9010022. PMID: 31861911 PMCID: PMC7019839. https://pmc.ncbi.nlm.nih.gov/articles/PMC7019839/
